Abstract
Background: The periodontium is a complex structural unit designed to support teeth and absorb masticatory forces within physiological limits. When these limits are exceeded, a state ofhyperfunction occurs, leading to potentially destructive changes in the toothsupporting tissues.
Objectives: This review article aims to analyze the etiology of periodontal hyperfunction, thehistological mechanisms of tissue response, and the clinical manifestations of occlusal overload.
Methods: This manuscript is narrative review focusing on physiological and pathological responses of the periodontium to occlusal hyperfunction. A comprehensive literature review was conducted, during which approximately 50 scholarly works were analyzed across major electronic research databases, including PubMed and Google Scholar. From this selection, specific studies most relevant to our thematic focus were prioritized, with a particular emphasis on contemporary data published between 2010 and 2024. Identifying even more recent materials that strictly align with the specific scope and objectives of this review article proved to be a significant challenge. The search strategy employed a combination of terms and keywords: “occlusal trauma”, “periodontal hyperfunction”, “alveolar bone resorption, “periodontal ligament”.
Results: Hyperfunction leads to the widening of the periodontal ligament space, alveolar boneresorption, and increased tooth mobility. The article explores the three phases of tissue reaction :active destruction, repair, and remodeling and differentiates between primary and secondary occlusal trauma.
Conclusion: Early diagnosis through specific methods and the elimination of causative factors (parafunctional habits and occlusal disharmony) are crucial for preventing irreversible damage and maintaining periodontal health.
Introduction
The periodontium is a structural complex composed of its constituent elements such as the gingiva, periodontal ligament, alveolar bone and tooth root cementum. These elements differ in anatomy and histology, but they share a common function that is vital to the masticatory apparatus.
The primary function of the periodontal structures is to support the tooth, anchor it to the alveolar bone, and absorb the forces acting upon the tooth and periodontium.
Due to its intrinsic function, anatomical and histological structure, biological plasticity and other properties, the periodontium is continuously subjected to various functional and non-functional loads. However, under normal conditions, these forces are adapted and have a positive effect up to a certain limit, defined as physiological limits. Once these limits are exceeded, a state of functional overload, or hyperfunction, ensues.
Hyperfunction of the periodontium has a negative and potentially destructive effect on the periodontium, the teeth and, more generally, the masticatory apparatus.
In this review article the causes of periodontal hyperfunction will be explained, the morphological changes that occur in the periodontal tissues, the mechanisms by which these forces act on the periodontium, and the clinical consequences of this condition, which are important for the diagnosis and treatment of cases in periodontal practice.
Forces And The Parodontium
The teeth and their periodontium are exposed to the action of various forces. Some forces are exerted during function, specifically during chewing, biting, swallowing, cutting, speaking, etc. These forces are beneficial, as the teeth and periodontal tissues themselves require forces and stimuli that promote the activation of the functions of the periodontal structures. [1]
Physiological forces are essential for maintaining the morphological integrity of the periodontium. These forces stimulate the metabolism of periodontal tissues, activate blood circulation, bone remodeling, the maintenance of periodontal width, and cellular activation (such as fibroblasts, osteoblasts, osteoclasts, cementoblasts, cementoclasts, immune cells), which produce extracellular matrix components, regulate structures by maintaining the balance between their formation and resorption. [2]
Besides physiological forces, which have a functional action, there are also non-functional forces acting on the periodontium, such as: teeth clenching, teeth grinding, inadequate interdental contacts, malocclusions, forces during inadequate orthodontic therapy, biting on various objects, incoordination and influence of the lip, cheek and tongue muscles.
All these forces, if they remain within physiological limits, that is to say if they are balanced or adapted by the resistance of the periodontium, are considered harmless. Negative consequences occur if these forces lie outside the physiological range.
The action of a force on the tooth and periodontium also depends on the quality of the force, which encompasses its intensity, duration, direction and point of application. If the forces are below the physiological limits, there will be a lack of stimulation of the periodontium and atrophic changes will occur. This condition is called hypofunction of the periodontium.
When occlusal forces exceed the physiological limits of the periodontium, the resulting damage is termed trauma from occlusion. This state is often associated with hyperfunction of the periodontium, where excessive, abnormal, or repetitive loads are placed on the teeth, exceeding their capacity to repair or adapt. [3]
Types of Forces and Characteristics
The characteristics of forces are: magnitude, duration, direction of action and point of application of the force. A force of moderate intensity does not cause periodontal damage if the periodontium is intact. If the periodontium is diseased, then even the application of moderate forces will affect the prognosis of the condition, namely by accelerating the destruction of the periodontium.
Meanwhile, all high-intensity forces will lead to the complete destruction of the periodontium. A force acting for a short period is more likely to produce reversible changes, whereas a force of lower intensity but longer duration causes greater damage.
Forces act in a vertical, horizontal or combined direction. Vertical forces act along the tooth’s axis and tend to intrude the tooth into the alveolus. The action of these vertical forces is counteracted by the inclined periodontal fibers.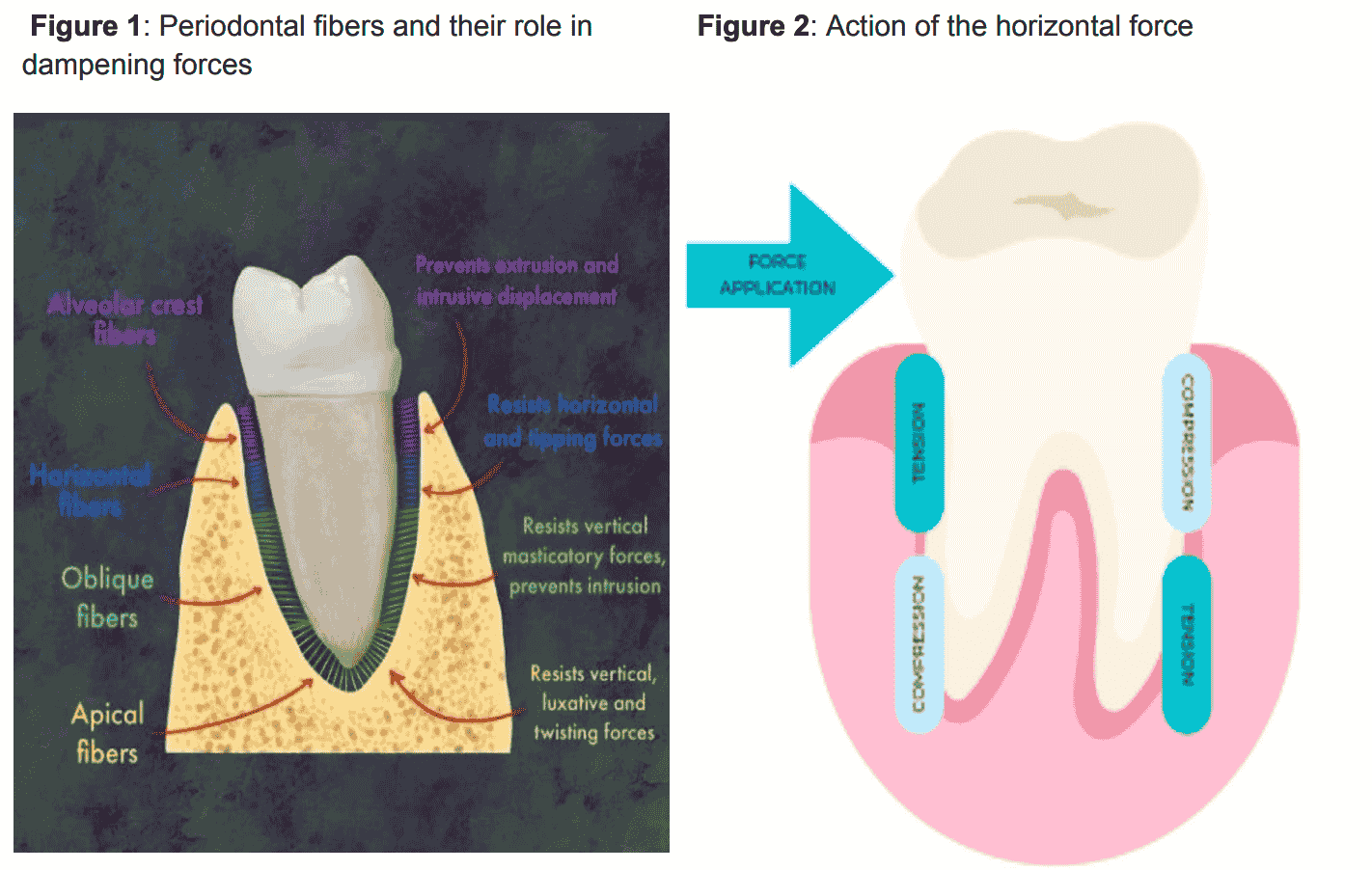
The Periodontal Ligament (PDL) functions as a complex biomechanical interface that anchors the dentition within the alveolar bone through a highly organized network of collagenous fibers, primarily Type I and III, which operate as a dynamic viscoelastic structure. This non-linear tissue is not merely a static connective medium but a specialized shock-absorption system that dissipates mechanical loads to protect the radicular structure from pathological concentrations of stress, effectively transducing physical stimuli into biochemical and cellular responses via mechanotransduction. When an external force is applied to the tooth, the PDL fibers undergo differential deformation, establishing specifictension zones where fiber elongation stimulates osteoblastic activity for bone apposition, and compression zones where fiber impaction triggers osteoclastic recruitment for localized bone resorption. The interstitial fluid within the PDL plays a critical role as a hydraulic damper, modulating the ligament’s resistance based on the magnitude and duration of the applied force, ensuring that the integrity of the fibrous matrix remains paramount for dental homeostasis. If the applied force exceeds the adaptive capacity of the PDL, it can lead to focal ischemia, hyalinization of the ligament, and potential root resorption, confirming that the primary physiological function of the PDL is to maintain a precarious equilibrium between mechanical stability and the biological plasticity required for the continuous remodeling of the periodontium. [4]
The transmission and distribution of forces also depend on the size, shape, cuspal inclination, tooth surface, contact with the agonist and antagonist, and the position of the tooth.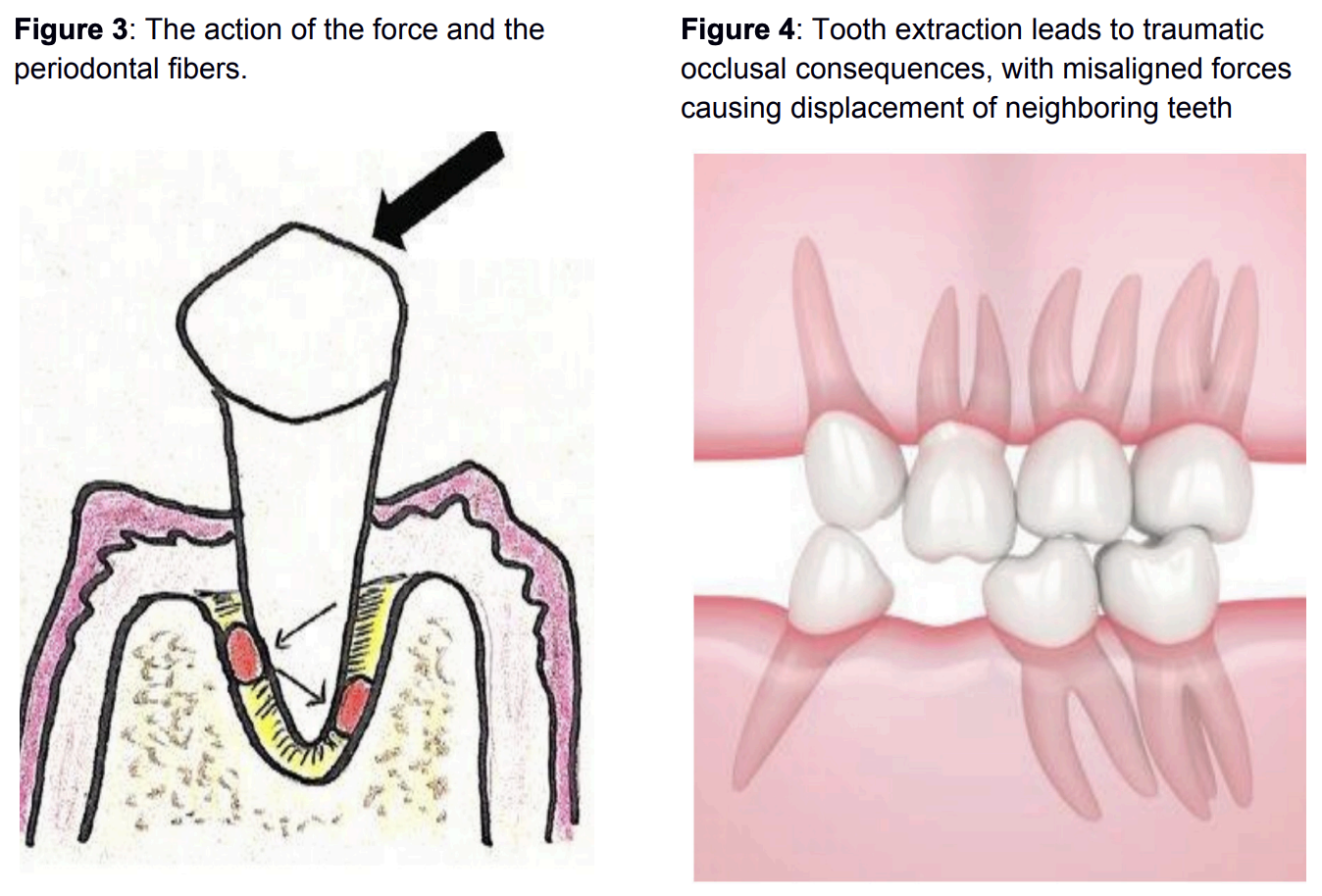
Hyperfunction of The Parodontium
First, let us explain the terms ‘traumatic occlusion’ and ‘occlusal trauma’. By ‘traumatic occlusion’ we mean an inappropriate occlusal contact between the teeth that damages the periodontium, the masticatory muscles and the temporomandibular joint. Meanwhile, ‘occlusal trauma’ refers to tissue injury caused by the impact of forces.
According to the manner in which the tissue reacts to the action of traumatic forces, we distinguish 3 phases:
1. The phase of active tissue destruction
During this phase, clinical and histopathological signs of occlusal trauma are present, indicating weak tissue unable to resist the action.
2. The adaptation phase
During this phase, the tissue’s structural organization is re-established, almost completely restoring the biological characteristics associated with the homeostatic behavior of the periodontal supporting component and the tissue’s resistance.
3. The Remodeling Phase
This phase then proceeds to meet the homeostatic requirements of the periodontal supporting tissues, establishing the final structural and architectural characteristics of the cementum, periodontal ligament and alveolar bone, with functional reorientation of the fibers of the periodontal ligament and the bone trabeculae, in accordance with the new functional requirements of the area.
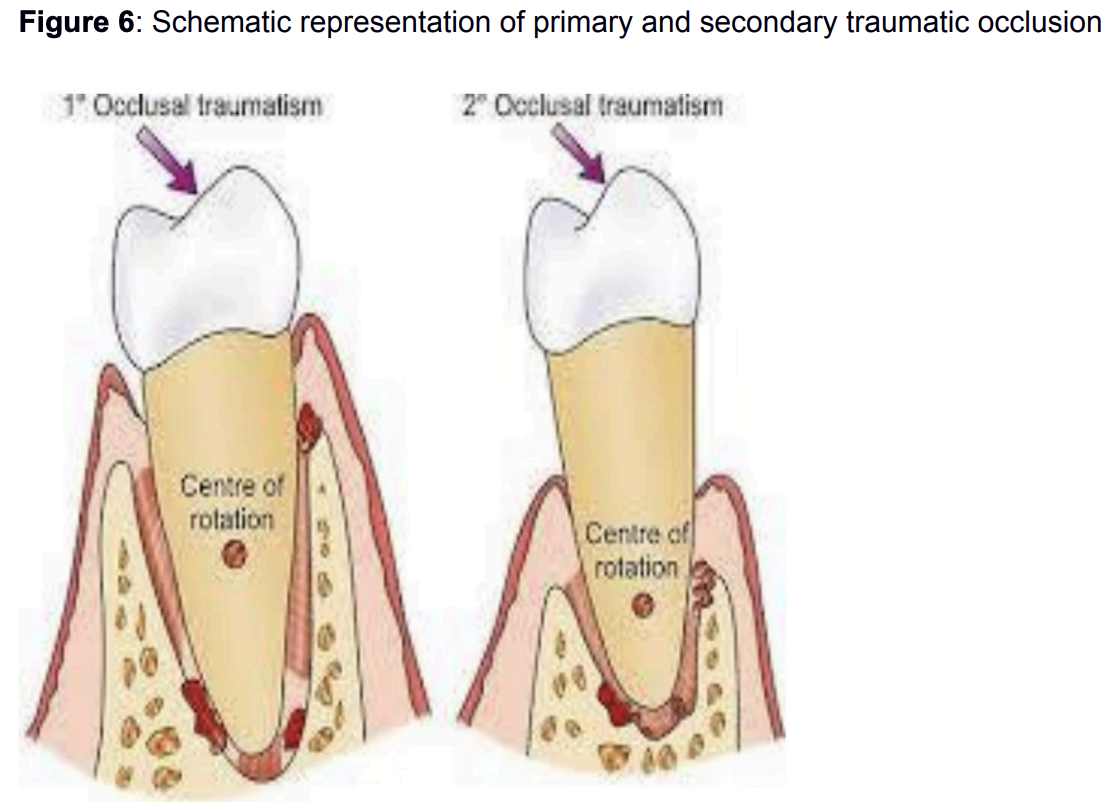
Occlusal trauma is divided into primary when forces act on a healthy periodontium and secondary when normal or increased forces act on a periodontium already damaged by periodontitis. [5]
Primary Traumatic Occlusion
Primary traumatic occlusion is the action of forces of expressed intensity on an intact periodontium. The changes in the periodontium resulting from the action of occlusal forces depend on the qualities of the force as well as the periodontium’s ability to adapt to these forces. Thus, the periodontium can adapt to the action of forces without sustaining damage, and conversely it may fail to adapt and exhibit changes resulting from periodontal injury
Adaptation of the periodontium by the action of forces of expressed intensity
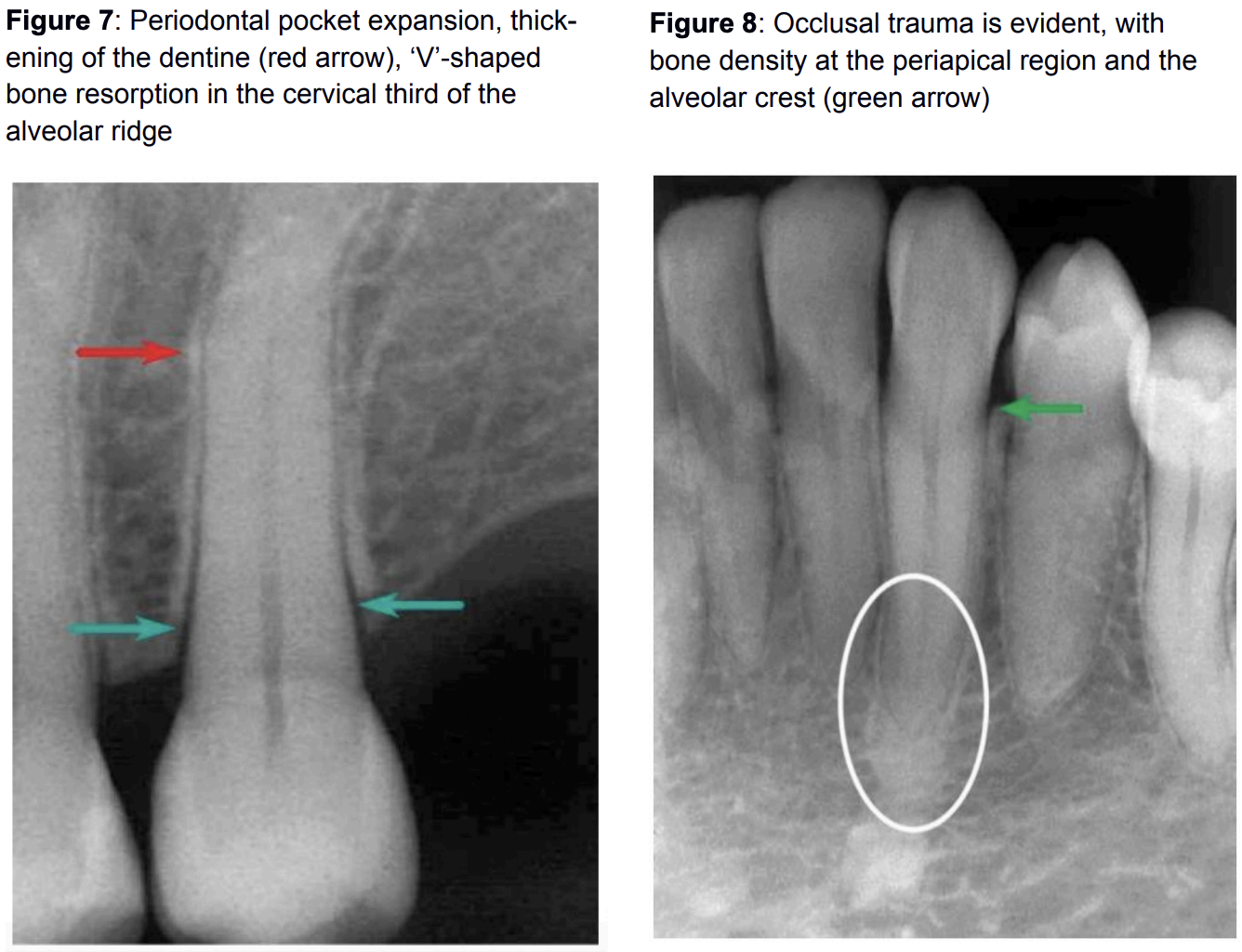
The adaptation of the periodontium by the action of forces implies the adaptability of the periodontal structures to new functional demands and their coping with them. This is achieved mainly through remodeling and expansion of the periodontal space. The periodontal ligament acts as a mechanical and hydraulic shock absorber. It is mechanical because, with the expansion of the periodontal space, the surface area for force distribution increases. This reduces the pressure exerted on the alveolar bone. A hydraulic shock absorber because the tissue fluid in the periodontal space allows for load absorption, and due to the periodontal expansion, fluid movement is enabled, thus allowing for tooth mobility within the alveolus.
Alveolar bone will increase in bone density but occlusal loading will further reinforce alveolar bone structure. Specifically, alveolar bone will have increased bone density and will develop a specific trabecular orientation only after occlusal loading, in order to distribute occlusal stresses. [6]
Unsuccessful adaptation of the periodontium
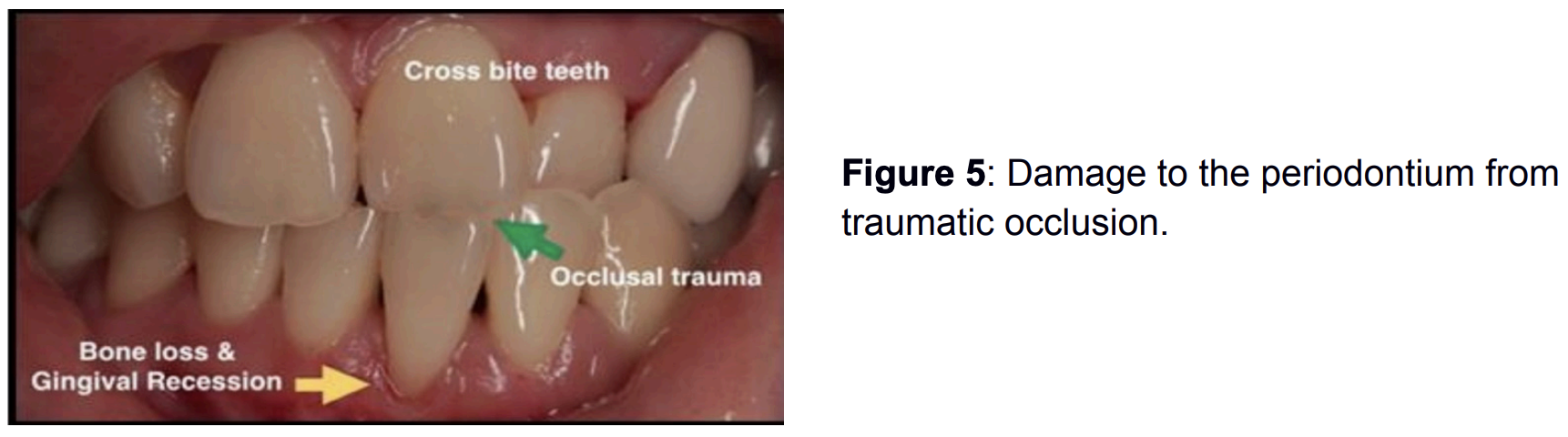
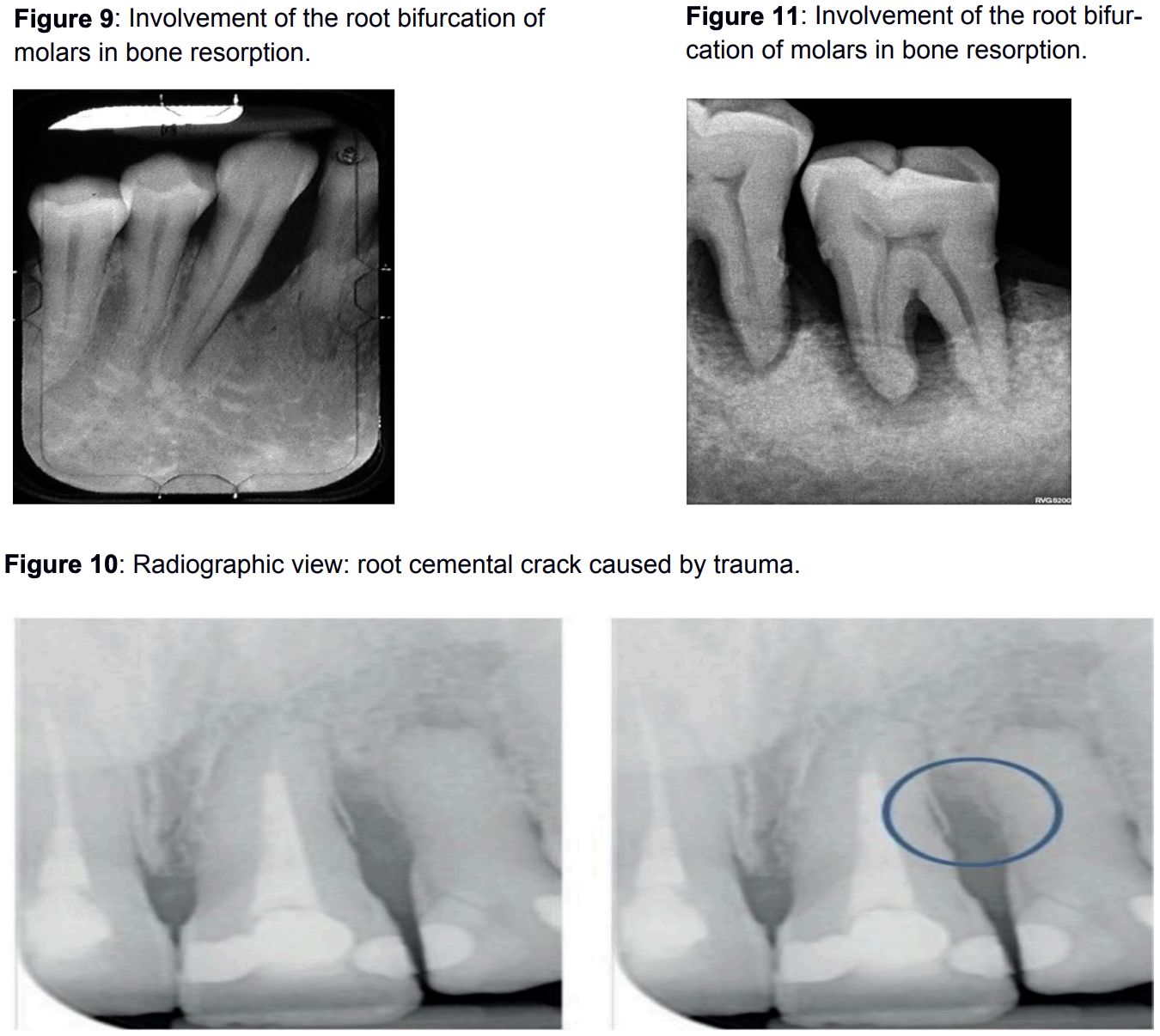
The periodontium cannot adapt when forces exceed its adaptive capabilities. Consequently, changes appear, such as an expansion of the coronal part of the periodontium in the form of a funnel, accompanied by bone resorption around the area. Bone resorption is most pronounced between the roots (furcations). Resorption of the root cementum also occurs. Clinically, these changes manifest as increased tooth mobility and pathological gingival sulcus depth.
The condition becomes even more severe and irreversible when there is existing inflammation of the periodontal tissues from dental plaque. When occlusal trauma is superimposed on an inflammatory state, the changes become irreversible and cannot be fully reversed, even if the traumatic force is eliminated. [5] As a result, the attached epithelium will migrate apically, creating a true periodontal pocket (primarily an infrabony pocket). Trauma accelerates bone resorption in an area already inflamed. As a result, there is an earlier reduction in bone height and the development of angular or crater-shaped bone defects, which no longer regenerate to their former level.
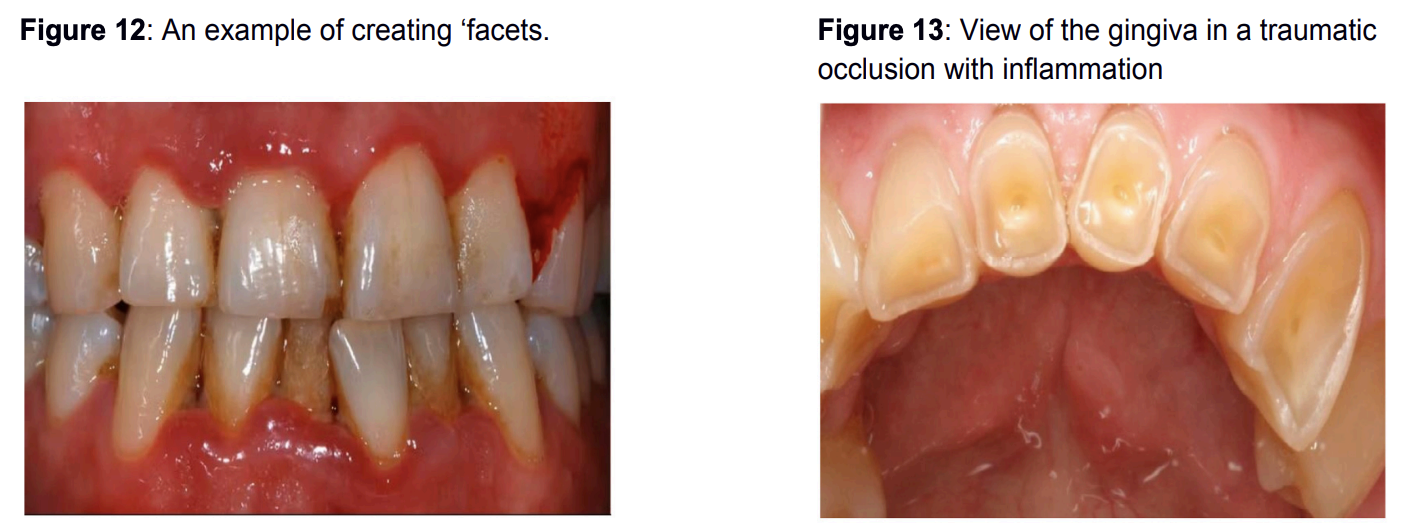
Due to occlusal forces and occlusal trauma, abrasion and inappropriate friction occur between the teeth, resulting in lustrous, flattened areas on the tooth enamel, particularly on the occlusal and incisal surfaces. These teeth in traumatic occlusion may be sensitive to percussion and suffer from chronic pain.
Secondary Traumatic Occlusion
Secondary traumatic occlusion refers to irregular tooth contact caused by the action of forces on a previously diseased or damaged periodontium of the same etiology. In cases of secondary occlusal traumatism, the periodontium is in a more severe condition and adaptation is almost impossible.
Thus, in these teeth the support is compromised, and even normal functional forces can exacerbate the condition. It differs from primary occlusal trauma, where the tooth support is healthy.
They are characterised by marked bone resorption and increased mobility, altered tooth position, pain on chewing, gingival bleeding and inflammation.
Conclusion
In conclusion, a traumatic occlusion and a state of periodontal hyperfunction should not be based solely on the appearance of the relationships between the teeth and the jaws. A traumatic occlusion must be confirmed by identifying the changes and signs of occlusal traumatisation, or of periodontal hyperfunction. There are various cases in which a traumatic occlusion is suspected, yet it actually proves to be balanced because a harmonious habitual occlusion has been established. There is also the other side, where the intermaxillary relationships are harmonised but there is periodontal damage. Detecting signs of traumatic occlusion through specific diagnostic methods and administering targeted treatment.
References
- Rajendran, M., Mahalakshmi, A., Selvam, A. et al. Interplay of occlusal forces and the periodontium. J. Stomat. Occ. Med. 8 (Suppl 1), 17–24 (2016).
- Wang, T. , Liu ,X., Li, J. , Yue, Y., Li, J.,Wang, M. , Wei, N.,Hao,L. Mechanisms of mechanical force in periodontal homeostasis: a review. Front. Immunol., 16 August 2024. Volume 15 - 2024
- J Indian Soc Periodontol. 2018 Sep-Oct;22(5):395–400.
- McCormack SW, Witzel U, Watson PJ, Fagan MJ, Gröning F. The biomechanical function of periodontal ligament fibres in orthodontic tooth movement. PLoS One. 2014 Jul 18;9(7):e102387.
- Fan. J, Caton. J, Occlusal trauma and excessive occlusal forces: Narrative review, case definitions and diagnostic considerations. Journal of Periodontology, 21 June 2018.
- Yeh KD, Popowics TE. The impact of occlusal function on structural adaptation in alveolar bone of the growing pig, Sus Scrofa. Arch Oral Biol. 2011 Jan;56(1):79-89.
Disclaimer / Publisher’s Note:
The statements, opinions, and data presented in all publications are solely those of the individual author(s) and contributor(s) and do not necessarily reflect the views of YellowMark Publishing House, the journal, or the editor(s). The publisher and editor(s) disclaim any responsibility for any injury to persons or property resulting from any ideas, methods, instructions, products, or procedures referred to in the content.
© 2026 Author(s). Published by YellowMark
This article is distributed under the Creative Commons Attribution License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.